Freitag, 26. November 2021
-
07:30 – 08:15
Registrierung
-
08:00 – 09:30
Vortragssaal 2
Strahlenschutz in der Handchirurgie: Veranstaltung zur obligatorischen Rezertifizierung
S. Schindele, Zürich (CH)Einführung und Information
S. Schindele, Zürich (CH)
Einführung in den Strahlenschutz
R. Simmler, Zürich (CH)
-
08:15 – 09:30
Gartensaal 1 A-C
Gong Show
D. Merky, Bern (CH) / C. Wirtz, Chur (CH)Determining diagnosis of scaphoid healing with cone beam CT after six weeks of immobilization
B. Moutinot1, C. Bouvet2, J. Y. Beaulieu1, S. Boudabbous1 (1Genève; 2Sierre)
Show text
Purpose : To assess the accuracy and reliability of using cone beam computed tomography (CBCT) compared to X-ray six weeks after injury for predicting scaphoid union.
Materials and methods Overall; 52 patients with scaphoid fractures between April 2018 and March 2019 were prospectively included in this study. The mean age was 34.52 (13–88) years, and the gender ratio male/female 43/9. Of the fractures, 26 had occurred on the right side, and 26 on the left side. In total, 28 % of patients were manual workers. All patients underwent X-ray and CBCT six weeks after injury. Four readers, two radiologists, and two hand surgeons analyzed the findings using double-blinded X-ray and CBCT and categorized fractures as consolidated based on a 50 % visibility threshold concerning trabecular bridges. Proximal pole sclerosis, communition, cyst formation, and humpback deformity were similarly analyzed for all cases. Agreement between readers was calculated using Kappa, and sensitivity, specificity, and accuracy using RStudio software. The gold standard was the radiologic and clinical follow-up for all patients at two months.
Results Inter-reader agreement between the four readers was moderate concerning X-ray (0.543) but substantial concerning CBCT (0.641). It was almost perfect between seniors regarding CBCT (Kappa = 0.862). Sensitivity, specificity, and accuracy were 0.75–0.78, 0.4, and 0.61–0.64, respectively, for two readers regarding CBCT. The X-ray values were 0.65–0.71, 0.35–0.4, and 0.53–0.59, respectively.
Conclusion CBCT proves more accurate and reliable than X-ray for diagnosing scaphoid union at an early follow-up and prevents longer immobilization and interruption of activity or work.
Treatment of osteochondromas in the forearm of children
J. Mercier1, R. Bernasconi1, C. Steiger2, A. Kaempfen1, A. Krieg1 (1Basel; 2Geneve)
Show text
Osteochondromas are benign bone tumors, which stop growing at skeletal maturity. Different ways to treat osteochondromas of the forearm exist for children. Foremost the conservative therapy for children with no pain, no functional disabilities or no esthetical problems. For children with symptoms or deformities a surgical procedure is to consider. A simple excision can be done or a bone lengthening can be planed. Various studies have been carried out to determine the best treatment method for osteochondromas of the forearm describing different surgical techniques but no consensus has yet been found. In this retrospective study we used the data of 18 patients (a total of 24 forearms), who have been treated in Universität Kinderspital beider Basel (UKBB). The purpose was to compare the radiological and functional outcome in patients with osteochondroma of the distal radius and ulna after a surgical excision (with or without bone lengthening) and to compare them to those treated conservatively, to determine the best treatment plan. Our study has shown a significant improvement of the function and the cosmetic appearance of the forearm after an operative procedure, independently from bone lengthening. We observed among others an increase in wrist and elbow mobility with decrease of pain and a confirmed high cosmetical satisfaction for the majority of the patients. In conclusion there is no indication for an operative treatment in symptom free patients who are able to perform tasks of daily life. However, if a patient suffers from functional impairment or pain, an operative approach is recommended. This treatment assures high patient satisfaction with improved clinical function, better cosmetic outcome and partially improved radiological parameters. The functional outcome is the same with or without bone-lengthening.
Early results of interleukin-1 receptor antagonist in treating calcific periarthritis of the hand
A. Durdzinska Timoteo1, S. Durand1 (1Lausanne)
Show text
Introduction
Calcific periarthritis is an idiopathic disease predominant in women around 45 years, with a rapid-onset, severe, monoarticular, atraumatic pain, local inflammation and a round, amorphous calcification on X-ray. Although only 2% occur in the hand the spontaneous resolution is slow: 3 weeks to 18 months. Current treatment options are full dose NSAID (non-steroid anti-inflammatory drugs) that lead to resolution of pain in 10 days or steroid infiltration. One alternative could be anakinra, an antagonist of interleukin-1 receptor, that proved safety and effectiveness in crystalopathies and calicific periarthritis of the shoulder. We present a pilot study on effectiveness of anakinra in treatment of hand periarthritis.
Materials and methods
In 2020, we treated 8 female and 2 male patients with mean age of 45 (range 29-55) with daily subcutaneous abdominal injections of 100mg anakinra until the pain relief. Additional paracetamol was allowed, but no splint or NSAID. We controlled the patients every day until pain relief, then at 1 and 3 weeks. Primary assessment factor was pain measured by VAS. Secondary assessment factors were: range of motion (ROM) measured by a goniometer; temperature by a laser surface thermometer (Visiofocus PRO); redness by DermaCatch; hypervascularisation qualified in ultrasonography; oedema – defined as the distance between the bone and skin surface in the ultrasound. A control X-ray was made at 7 and 21 days to see changes in calcification. All the data was analysed by Wilcoxon test.
Results
Patients received from 1 to 5 doses, mean 2.7. The pain (at presentation mean 4.95, SD 2.43) decreased significantly at day 2 (mean 1.1, SD 1.35, p=0.014). The difference was statistically significatif at day 2 for ROM (p=0.015), redness (p=0.0625) and oedema (p=0.093) and at day 3 for temperature (p=0.031). The calcification diminished the size and density in 8 and disappeared in 2 cases. There was no adverse effect.
Discussion, conclusions
There were 4 limitations: small group, no reference group, reliability of measurements by ultrasound and DermaCatch, loss of some controls due to covid. This pilot study showed safety, fast results with significant pain and inflammation decrease after 2 doses, that confirm the first results seen in shoulder periarthritis. Anakinra can shorten pain and work absence period, be an alternative treatment in patients with NSAID contrindication and localisations that are not compatible with steroid infiltration.
Distal Phalanx Fractures After 1-Year: The Good, The Bad, and The Ugly
C. S. Bratschi1, C. Kammerhofer2, F. Mauler2, T. Ly2, C. Meuli-Simmen2, A. Weber3 (1Baselland; 2Aarau; 3Zürich)
Show text
INTRODUCTION: Fractures occurring in the distal phalanx of the hand are very common. Luckily, most heal without lasting complications. However, some fractures can result in sequelae, such as chronic pain, disability, and nail dystrophy. However, there is scant published data regarding the long-term effects of these fractures on patients.
The study's primary aim was to identify predictors of a therapeutic outcome in patients with distal phalanx fractures. The primary outcome was the presence of symptoms related to the distal phalanx fracture one year after occurrence. The secondary aim was to describe which factors characterize patients with chronic pain, changes in sensation, functional limitations, or nail growth disturbances.
METHODS: A cohort, single-center study was performed. Patient records were retrospectively extracted, and follow-up was prospectively evaluated via examination, radiograph, and questionnaire responses.
Inclusion: Adults treated for a distal phalanx fracture of the hand between 2015 and 2019.
Exclusion: Patients lacking significant evaluable records or those with a bony avulsion of extensor or flexor tendon.
Primary Outcome: Presence of symptoms at least one year after trauma.
Secondary Outcomes: Age, sex, severity of pain, digits affected, activities of daily living, hand dominance, fracture type, type of therapy (surgical and nonsurgical), hand immobilization (weeks), inability to work (weeks), range of motion, dystrophic changes of the nail, changes in sensation, and scoring on a standardized instrument (Disabilities of Arm, Shoulder, and Hand - composite, work and hobby).
RESULTS: A total of 128 patients were included. After one year, most patients experienced ongoing symptoms (54%). Chronic pain occurred in 39% of patients in the symptomatic group. Sensory changes were found in 83% of symptomatic patients. Inability to work was identical (mean = 6 weeks) in both groups despite differences in functional disability (DASH and subset scoring).
DISCUSSION: Patients in the symptomatic and asymptomatic groups were both able to return to work in a similar length of time. Additionally, there is a congruence between symptomatic patients, functional deficits, and changes in sensation. As expected, open fractures were more likely to result in nail growth disturbances. Interestingly, this effect was most pronounced in the middle finger.
Outcome prediction by Diffusion Tensor Imaging (DTI) in patients with traumatic median nerve injury
T. Voser1, S. Durand1, F. Becce1, M. Martin1, T. Kuntzer1 (1Lausanne)
Show text
Introduction
Accurate quantification of peripheral nerve axonal regeneration after injury is critically important. Current strategies, including clinical assessments and neurophysiological studies, are limited to detecting early reinnervation. DTI is an MRI modality which assesses the water molecules’ diffusion in a tissue. In anisotropic tissues, such as peripheral nerves, the water diffusion is greater in some directions than in others. Fractional anisotropy (FA) decreases with axonal degeneration and increases with axonal regeneration. The aim of this pilot study is to evaluate peripheral nerve DTI as a potential predictive factor of clinical outcome after median nerve section and microsurgical repair.
Materials and methods
Between 2017 and 2020, we included 10 patients (9 males, 1 female; mean age, 38.6 years) with complete section of the median nerve, who underwent microsurgical repair up to 7 days after injury. The minimum follow-up period was 1 year, with regular clinical visits including Rosen Lundborg score. Electroneuromyography was performed at 3 and 12 months. DTI MRI of the injured wrist was planned at 1, 3 and 12 months (M1, M3 and M12). The main endpoint is the comparison of DTI values (FA) at 1, 3 and 12 months after surgery with the final clinical outcome. The FA values were measured by two observers, centered at the level of the suture with a coverage of ± 1cm (7 MRI sections). The comparison of FA values was done using one-way ANOVA.
Results
The M1 and M3 DTI MRI were performed in all patients, while the M12 DTI MRI in 8/10 patients. Rosen Lundborg score at M12 was obtained in 8/10 patients. The mean (SD) FA values at M1, M3 and M12 were 0.327 (0.035), 0.353 (0.032), and 0.438 (0.063) respectively. This increase is statistically significant (p=0.0001). The mean (SD) Rosen Lundborg scores at M3, M6 and M12 were 1.20 (0.42), 1.45 (0.45), and 1.69 (0.50) respectively (p=0.097). Interobserver reliability of FA measures was excellent (ICC= 0.802).
Discussion
The DTI modality is a safe, pain free, quantitative, and reproducible technique. We note signs of nerve regeneration after microsurgical repair of the median nerve, objectively quantified by the statistically significant increasing FA values. Additional analyses are currently underway to determine if cut-offs could be set to either predict a promising nerve regeneration or the need for an eventual surgical revision.
Six-strand flexor pollicis longus tendon repairs with and without circumferential sutures
G. Lautenbach1, M. Guidi1, B. Tobler-Amman2, V. Beckmann-Fries1, E. Oberfeld2, L. Schrepfer 3, S. H. Hediger3, A. Kämpfen 3, E. Vögelin2, M. Calcagni1 (1Zürich; 2Bern; 3Basel)
Show text
ABSTRACT
Background: Several different suture techniques are currently used for flexor pollicis longus tendon repairs. In the search for an optimal outcome authors began to omit the circumferential suture.
Method: A six-strand core suture technique with (33 patients) and without circumferential sutures (16 patients) was used. Afterwards the wrist was stabilized with a dorsal blocking splint and a controlled early active motion protocol was applied. Data on demographics, type of injury, surgery, postoperative rehabilitation and outcome measurements were collected at weeks 6, 13 and 26.
Results: We report the outcomes of flexor pollicis longus tendon repairs with and without circumferential sutures in 49 patients. There were no significant differences in thumb range of motion and strength between the two treatment groups. Both groups expressed similar satisfaction with the surgical treatment.
Conclusion: Six-strand repair technique is an effective procedure to assure early active motion after flexor pollicis longus tendon injuries and the use of the circumferential suture is not essential to achieve good results.
Union is strength – don’t underestimate the force of tendons to possibly maintain nonunion
L. Fuest1, L. Noser1, E. Vögelin1 (1Bern)
Show text
Introduction
Known complications of joint arthrodesis are malalignment, implant failure, delayed union or nonunion. Underlying reasons for the latter can be patient specific (smoker, diabetes, malcompliance) or due to insufficient fixation or immobilization.
Case report
We present a 51 year old male pastor who suffered a traumatic scapholunate ligament (SL) rupture in both hands in 2008 resulting in a symptomatic SLAC (scapholunate advanced collapse) wrist due to failed dynamic stabilization in both wrists. A total of 14 operations were necessary to accomplish joint union at the left wrist. Therefore, the treating surgeons directly opted for a total wrist arthrodesis on the right side in 2016. But alas 7 months postoperatively, a painful wrist articulation persisted. A CT scan confirmed union of the lateral column with nonunion of the central column and incomplete union of the medial column Revision surgery with additional STT (scaphotrapeziotrapezoidal)-fusion and bone allograft between capitate and hamate was performed in 2017 resulting in persisting symptomatic nonunion of the STT-joint. Additional revision surgery of the STT fusion included a femur allograft interposition in 2019 and with pridie drilling in 2020. A Spect-CT scan in 08/2020 confirmed a complete union of the central column but persistent nonunion at the STT fusion site.
The patient continued to report possible and painful nodding motion upon activation of the FCR and ECRL tendons. This led to the assumption, that micro-movements due to the mechanical force transmission of the flexor and extensor tendons at the insufficiently healed union between 2nd metacarpal bone, trapezium and trapezoid were the underlying cause hindering bone fusion.
Ultimately, revision surgery of the STT nonunion with an iliac allograft and tenotomy of the FCR and ECRL tendons was carried out. Six weeks postoperatively, the patient was pain free for the first time and the CT-scan confirmed consolidation.
Conclusion
With the tenotomy of the ECRL and FCR tendons, the mechanical force transmission at the fusion site could finally be interrupted and thus, permitted the necessary mechanical stability to heal. In cases of persisting nonunion, potential transmission forces as underlying causes for nonunion should be searched and excluded.
Ein handchirurgisches "Armageddon".. .oder der lange Weg zur minimalen Handfunktion
F. Fiumedinisi1, T. Giesen1, E. Fritsche1 (1Luzern)
Show text
Einleitung
Eine 5 Fingeramputation der dominanten Hand gehört neben Explosionsverletzungen wohl zu den schwersten Handverletzungen, die man sich zuziehen kann, insbesondere wenn es sich dabei um keine scharfen Amputationen, sondern um Avulsionsamputationen handelt. Diese Art der Verletzung stellt die behandelnden Chirurgen vor grösste Herausforderungen in der Planung und Ausführung der langwierigen Behandlung. Dabei müssen alle Register der Behandlungsoptionen herangezogen werden. Diese Herausforderung verlangt Know-How und Erfahrung an spezialisierten handchirurgischen Zentren. Wir berichten über die Primärversorgung und Folgeeingriffe eines wirklich seltenen Falles.
Fallbericht
Ein solches Armageddon ereignete sich bei einem 42 jährigen, handwerklich tätigen Linkshänder, als er stolperte und sich mit der linken Hand auf einem Heubläsegerät abstützen wollte. Dabei kam es zu einer Avulsionsamputation aller Finger der dominanten linken Hand auf Grundgliedhöhe. Wir haben uns für eine sehr aufwändige, mehrstufige und anspruchsvolle Behandlungsstrategie entschieden. Die Primärversorgung bestand aus der orthotopen Replantation des Daumens über eine freie ALT-Lappenplastik als chimäre Lappenplastik und der heterotopen Replantation des Mittelfingers an die SCIP-Gefässe der linken Leiste. Nach 3 Monaten konnte der Mittelfinger orthotop über den Lappenstiel eines Interossea-posterior Lappens rereplantiert werden. Wir zeigen die verschiedenen, teilweise sehr komplexen Schritte der rekonstruktiven Eingriffe auf dem langen Weg zur Rehabilitation auf. Der Patient erreicht eine überraschend gute Handfunktion nach diesem desaströsen Unfallereignis.
Diskussion
Der Fall zeigt exemplarisch auf, dass der Entscheid zur alleinigen Stumpfversorgung in diesem Fall keine Option war und sich somit mit dem Willen des Patienten deckte. Als Beispiel in der Gong Show soll er Motivation für die Kollegen sein, auch in fast "hoffnungslosen" Fällen, alle Register der Handchirurgie zu ziehen, um wenigstens eine minimale Handfunktion zu erreichen nach dem Motto: "Wenig Handfunktion ist besser als keine Funktion".

Unfallröntgenbild 1-2 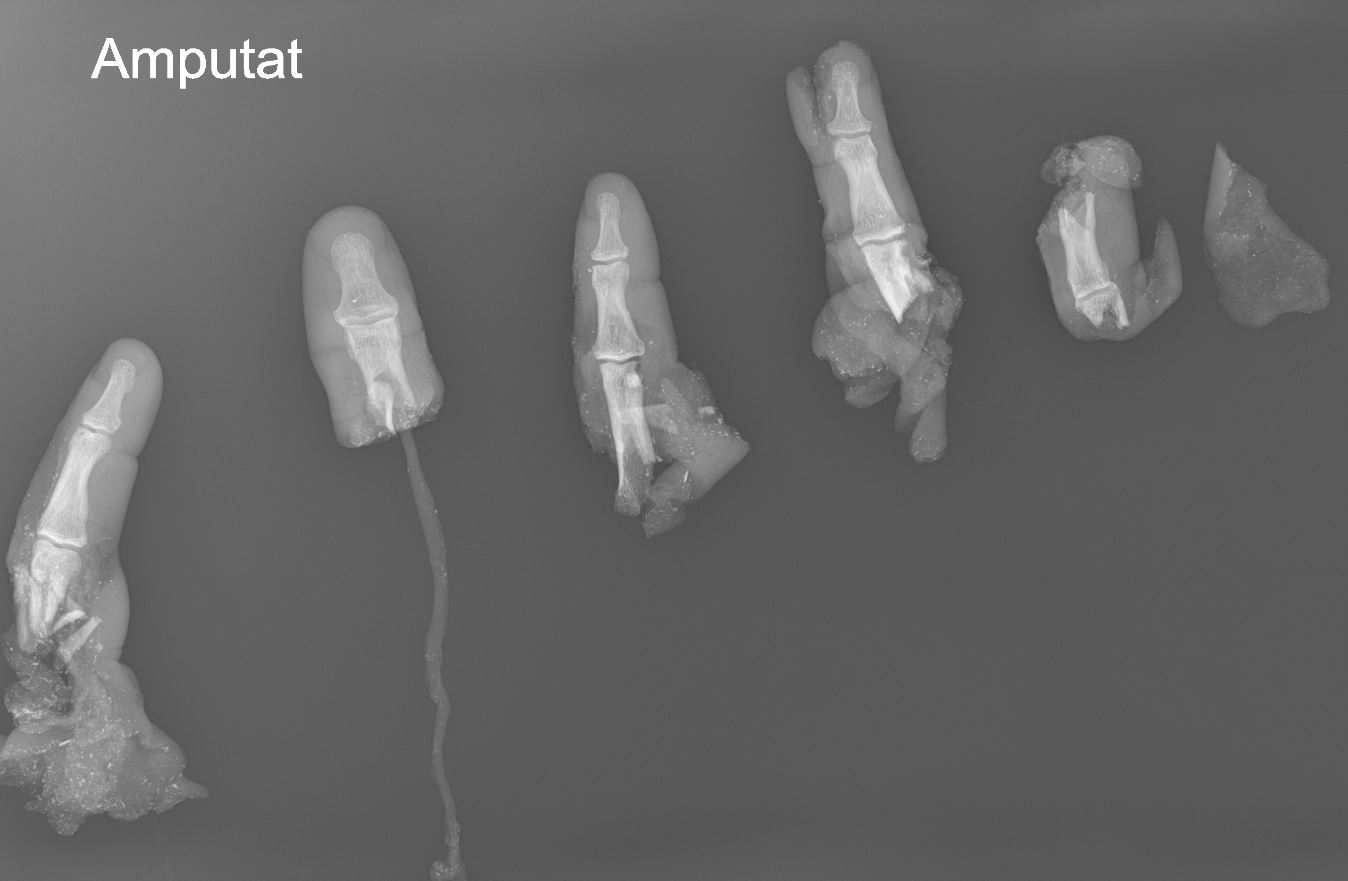
Unfallröntgenbild 2-2 Proximal median nerve reconstruction using wide awake tendon transfer and microsurgical nerve graft
A. Frey1, E. A. Kappos1, D. J. Schaefer1, A. Gohritz1 (1Schweiz)
Show text
Introduction: Functional reconstructive surgery in local anaesthesia using epinephrine as a chemical tourniquet (wide-awake approach) offers many advantages, in particular regarding patient cooperation during tendon transfer to optimise tension. However, this method may appear impossible when nerve reconstruction involving microsurgical nerve grafting is required.
Case report: A 17-year-old female suffered severe trauma to her right dominant arm during a motor vehicle accident requiring humeral plate osteosynthesis. Postoperative median nerve palsy was noted. As the origin of the nerve palsy remained unclear, the patient was referred to our service and ultrasound examination revealed a median nerve defect of 7 cm. Upon clinical presentation, the patient showed recovery of the intrinsic median nerve function of the thenar muscles, presumably due to nerve interconnections. However, thumb and index finger flexion and sensibility of median nerve territory were completely absent. As the patient’s primary goal was fast restoration of pinch and grasp, it was decided to combine forearm tendon transfer with nerve grafting for high proximal median nerve reconstruction.
Results: Successful tendon transfer was achieved using wide-awake approach for optimal intraoperative adaption of tendon tension during brachioradialis-to-flexor pollicis longus transfer and side-to-side suture of FDP 2-to-3. Microsurgical median nerve reconstruction was later performed by sural nerve grafts under general anesthesia.
The patient started hand therapy 3 days postop and was able to return to work at 50% capacity already 6 weeks after surgery and full capacity after three months. Almost two years postoperatively, the patient has resumed full work and leisure activity with acceptable sensibility which is still improving.
Conclusions: Wide-awake surgery in local anaesthesia offers great advantages during tendon transfers, especially regarding optimization of tension. It can be safely combined with procedures in general anesthesia during complex nerve reconstructions, as shown in the presented case.
Fixierte Subluxation des distalen Radio-Ulnar-Gelenkes infolge Malunion des Processus styloideus ulnae
S. C. Brackertz1, L. Reissner1, A. Schweizer1, L. Nagy1 (1Zürich)
Show text
Distale Radiusfrakturen und deren Begleitverletzungen führen häufig zu Problemen des Radio-Ulnar-gelenkes (DRUG). Malunionen des distalen Radius sowie Läsionen des TFC sind anerkannte Ursachen für Fehlstellungen, Instabilität und Beweglichkeits-Einschränkung des DRUG’s.
In den vergangenen 12 Jahren haben wir 4 Patienten mit einer fixierten Subluxation des distalen Radio-Ulnar-Gelenkes (DRUG) und aufgehobener Supination aufgrund einer Malunion des Processus styloideus ulnae (PSU) behandelt.
Im Gefolge einer distalen Radiusfraktur mit Abriss des PSU bestand keine wesentliche / ursächliche Fehlstellung des distalen Radius sondern lediglich eine Malunion des PSU. Durch eine Korrekturosteotomie des PSU konnte die Subluxation beseitigt sowie die Vorderarmrotation wiederhergestellt werden.
Die präoperativen Befunde betrugen im Mittel:
Pronation 75° (60-90°), Supination -8.75° (-50-25°) DRUG-Subluxation 47.5% (37-60%), die Fehlstellung des Ulnastyloids: 30.5° (2.5-50°) und 7.8mm (5.3-10.6mm)
Die postoperativen Befunde betrugen im Mittel:
Pronation 59° (45-70°), Supination 58° (40-85°) DRUG-Subluxation 8.5% (8-9%)
Malunionen des PSU können alleinige Ursachen einer fixierten Subluxation und des Ausfall der Supination darstellen und durch Korrekturosteotomien der PSU erfolgreich angegangen werden.
Rotational/Axial Deformity as Possible Complication in Distraction Lengthening in Brachymetacarpia
K. Kasparkova1, T. Sánchez1 (1Olten)
Show text
Abstract
Brachymetacarpia is a condition characterized by a shortened metacarpal that is caused by early closure of the epiphyseal plate which mechanism is unknown. The correction for brachymetacarpia is usually for cosmetic reasons as this condition does not usually impair function. The literature reports several different approaches for digits lengthening, including single-stage lengthening and rapid distraction with a bone graft. However, gradual distraction is the preferred method due to excellent cosmetic outcomes and
afew postoperative complications. We report report 3 cases (2 patients) of brachymetacarpia treated with distraction lengthening with postoperative 2 rotational/axial deformities as possible complications of this method.The first patient presented with bilateral brachymetacarpia and was surgically treated on the left side with no complications, on the right side with axial deformity due to loosening of external fixator in the course. Correction osteotomy was performed with excellent results and a satisfied patient with full range of motion. The postoperative course was uneventful, with no complications.
The second patient presented with rotational deformity after distraction lengthening of MC- V (extern). Correction osteotomy was performed with no complications and our patient was also satisfied with full range of motion.
Although callus distraction in the hand requires a long treatment period and it usually entails a relatively high rate of complications, it remains effective in achieving adequate bone length.results. Corretion osteotomy appears to be effective in axial/rotational deformities to achieve adequate cosmetic and functional results.
-
08:15 – 09:30
Gartensaal 2
Freie Mitteilungen III
V. Beckmann-Fries, Zürich (CH) / S. Rosca-Furrer, La-Chaux-de-Fonds (CH)Nachbehandlung bei proximalen Interphalangealgelenks (PIP)-Luxationsverletzungen
N. Pfister1 (1Wallisellen)
Show text
Motivation
Fingerluxationen treten im Alltag, vor allem bei sportlichen Aktivitäten häufig auf (Müller-Seubert, 2017). Trotz des verbreiteten Vorkommens werden die proximalen Interphalangealgelenks (PIP)-Luxationsverletzungen oft unterschätzt da die Weichteilverletzungen auf einem Röntgenbild nicht sichtbar sind (Paschos et al., 2014). Auch in meiner Institution werden häufig Klienten mit PIP-Luxationsverletzungen behandelt und es gab bisher keine einheitlichen Nachbehandlungsguidelines, was ich mit meiner Arbeit ändern wollte.
Methodologie
Es wurden die Nachbehandlungsguidelines von anderen Schweizer Spitälern evaluiert. Danach wurde eine Literaturrecherche zu der aktuellen Forschungslage in der „Cochrane Library“ und auf „PubMed“ durchgeführt. Daraus wurden hausinterne Guidelines erstellt.
Ergebnisse
Es herrscht Uneinigkeit bezüglich der Nachbehandlung. Die Mehrheit der Studien empfiehlt bei stabilen PIP-Luxationsverletzungen die Nachbehandlung mit Buddytapes, teilweise in Kombination mit einer Extensionsblockschiene oder Ruhigstellung. Jedoch wird nur wenig auf das genaue Nachbehandlungsprocedere eingegangen. Bei dem Austausch mit den hausinternen Ärzten fiel die Entscheidung auf die Nachbehandlung mit Buddytapes in Kombination mit einer Nachtlagerungsschiene, wie auch in der Studie von Lunger et al. 2017 erwähnt.
Implikationen
Die erarbeiteten Nachbehandlungsguidelines werden nun in einer Pilotphase von einem halben Jahr umgesetzt. Danach werden die Behandlungsergebnisse evaluiert.
Literatur im Abstract erwähnt:
Lunger, A., Lunger, L., Bach, A., Frey, C., Jandali, A.R., Sproedt, J. (2017). Frühfunktionelles Management bei Hyperextensionstraumata des proximalen Interphalangealgelenkes mit Läsion der palmaren Platte: Extensionsblock versus Achterschlaufe. Handchirurgie, Mikrochirurgie, Plastische Chirurgie, 49(5), 297-303.
Müller-Seubert, W., Bührer, G., Horch, R.E. (2017). Fingerluxationen im PIP-Gelenk -Therapie einer sehr häufigen (Ball)Sportverletzung. Sportverletzung, Sportschaden, 31(3), 154-159.
Paschos, N.K., Abuhemoud, K., Gantsos, A., Mitsionis, G.I., Georgoulis, A.D. (2014). Management of Proximal Interphalangeal Joint Hyperextension Injuries: A Randomized Controlled Trial. The Journal of Hand Surgery, 39(3), 449-454.
Die muskuläre Rehabilitation des Handgelenks – von der Propriozeption zum kraftvollen Stabilisieren
U. Osterwalder1 (1Baden)
Show text
Motivation:
Für einen kraftvollen Handgriff ist ein stabiles Handgelenk unabdingbar (Ducan et al.2013). Bei einer Ruhestellung sind bereits nach kurzer Zeit Kraftveränderungen in der Muskulatur feststellbar, welche zu Atrophien führen können (Haas et al. 2011). Die daraus entstandene muskuläre Dysbalance schränkt den kraftvollen Einsatz der Hand ein. Um dieser Entwicklung entgegenzuhalten, muss der Kraftaufbau möglichst rasch in den Therapiealltag eingebaut werden. Das stellt uns HandtherapeutInnen vor Herausforderungen, denn es gibt kaum Heimprogramme, welche verschiedene Methoden und angepasste Trainingsintensitäten beinhalten.
Fragestellung:
Welche rehabilitativen, evidenzbasierten Trainingsmethoden eigenen sich, um die muskulären Handgelenksstabilisatoren ohne grossen Aufwand zu Hause zu trainieren? Wie intensiv muss trainiert werden, damit die Kraft möglichst effizient gesteigert werden kann?
Methodologie:
Die Literaturrecherche wird in verschiedenen Datenbanken (Pubmed / GoogleScholar) und mittels Fachliteratur durchgeführt. Weil handspezifische Forschungsarbeiten zum Thema Kräftigung kaum vorhanden sind, muss die Literatur teilweise auf die Handgelenksstabilisatoren angepasst werden.
Ergebnisse:
Hagert (2016) erwähnt, dass die propriozeptive Gelenkskontrolle eine wichtige Bedeutung bei der Handgelenksstabilisation hat und deshalb in die Kräftigungsübungen integriert werden soll. Weiter sind isometrische und dynamische ex- und konzentrische Übungen wichtig für die Stabilisierung (Freiwald et al. 2016).
Implementierung:
Das Heimprogramm beinhaltet einen Leitfaden für den Trainingsaufbau und vier Trainingsmethoden, welche alle muskulären Stabilisatoren des Handgelenks berücksichtigt. Es ist mit einfachen Mitteln nach Instruktion der HandtherapeutIn, zu Hause durchführbar.
An einem Patientenbeispiel veranschauliche ich Ihnen mein Vorgehen.
Literaturverzeichnis:
- Ducan, S.F.M., Saracevic, C.E. & Kakinoki, R. (2013). Biomechanics of the Hand. Hand Clinics 29(4):483-92
- Haas, H.J. & Schmidtbleicher, D. (2011). Rehabilitation und Training. In Bant, H., Haas, H.J., Orphey, M. & Steverding, M. (Hrsg.), Sportphysiotherapeut (S.200-203, 262-274). Balingen: Spitta Verlag GmbH
- Hagert, E., Lluch, A. & Rein., S. (2016). The role of proprioception and neuromusculaar stability in carpal instabilities. The Journal of Hand Surgery, European Volume 41(1):94-101
- Freiwald, J.& Greiwing, A., (2016). Optimales Krafttraining Sport-Rehabilitation-Prävention. Balingen: Spitta Verlag GmbH
Die Touch-Prothese am Daumensattelgelenk aus Sicht der Handtherapie
C. Schneider1, N. Ziegler-Hollenstein1 (1Zürich)
Show text
Introduction :
Les douleurs résistantes à la thérapie situées autour de l’articulation trapézo-métacarpienne arthrosique peuvent être traitées par différentes procédures chirurgicales. L’arthroplastie par résection et interposition, lors de laquelle le trapèze est ôté et remplacé par un tendon, par exemple le fléchisseur radial du carpe (flexor carpi radialis), est considéré comme le goldstandard1,2. Depuis trois ans, notre clinique réalise toutefois l’implantation d’une prothèse (Touch, KeriMedical, Genève) lors d’arthrose isolée de l’articulation trapézo-métacarpienne. Il n’y a jusqu’à présent aucune littérature concernant la réadaptation et les résultats de cette opération. Le but de notre présentation est d’illustrer la rééducation après l’implantation d’une prothèse Touch par l’intermédiaire d’un exemple de cas et de présenter les résultats cliniques et subjectifs après six semaines post-opératoires.
Méthode :
Tous les patients ayant reçu une prothèse Touch dans notre clinique ont été documentés dans un registre prospectif. Les patients ont rempli la version courte du Michigan Hand Questionnaire (brief MHQ) et la force de préhension subtermino-latérale a été mesurée avant l’opération ainsi qu’à six semaines et trois mois post-opératoires. Lors du premier changement de pansement à deux ou trois jours post-opératoires, une attelle de pouce en néoprène a été mise en place et la mobilisation douce et sans charge du pouce a été expliquée. Le renforcement musculaire a débuté après les radiographies de contrôle (six semaines post-opératoires).
Résultats :
La plupart des patients ont été suivis en thérapie pendant six à huit semaines. Les résultats à trois mois post-opératoires sont actuellement disponibles pour 115 patients avec une moyenne d’âge de 63 (±8) ans. Avant la chirurgie, les patients avaient un score moyen de 46 (±14) à la version courte du MHQ. Six semaines plus tard, la valeur avait augmenté à 67 (±18; p≤0.001). La force de la pince subtermino-latérale se situait avant l’opération à 4.9 kg (±2.7). Après six semaines, les patients étaient au même niveau (5.0kg ±3.1; p=0.884).
Conclusion :
Le traitement après l’implantation d’une prothèse Touch est la plupart du temps sans complications et de courte durée grâce à un œdème limité, de faibles douleurs post-opératoires et une mobilisation précoce du pouce. Les patients sont souvent capables d’utiliser leur pouce de manière indolore après quelques semaines seulement et peuvent donc reprendre leurs activités quotidiennes comme le travail, le sport ou la musique.
Références bibliographiques :
1 Deutch Z et al. (2018). Hand (N Y), 13(4), 403-11
2 Wolf JM. et al. (2012). J Hand Surg Am, 37(1), 77-82
Handtherapie nach Einsatz einer MOTEC®-Prothese – erste Erfahrungen
A. Gisi1 (1Zürich)
Show text
Einführung
Komplexe Handgelenksverletzungen können zu arthrotischen Veränderungen im Radiocarpalgelenk führen und zu anhaltenden Schmerzen; resultierend in teils massiv eingeschränkten Funktionen im Alltag, Freizeit und Beruf. Eine der letzten chirurgischen Optionen ist die totale Versteifung. Eine Arthroplastik bietet eine Alternative für aktive Patient*innen, die ihre Handgelenksfunktion erhalten möchten (1). Im Gegensatz zu Knie- oder Hüftprothesen, welche seit langem zu Routineeingriffen gehören, sind Handgelenksarthroplastiken noch weniger ausgereift (2). Die MOTEC-Prothese ist eine Prothese der neusten Generation mit vielversprechenden Ergebnissen (1).
Ziel
Darstellung der handtherapeutischen Behandlung nach Einsatz einer MOTEC-Prothese anhand eines Fallbeispiels.
Methode
Eine Literatursuche zu Befunderhebung und Nachbehandlung bei Einsatz einer MOTEC-Prothese wurde durchgeführt. Anhand eines Fallbeispiels wird aufgezeigt, wie sich die Rehabilitation gestaltet und welche klinischen Verlaufs- und Ergebnismessungen durchgeführt wurden.
Ergebnisse und Implikation
In der Literatur wird eine sechswöchige Ruhigstellung mit anschliessendem Belastungsaufbau beschrieben. Als Ergebnismessungen werden Beweglichkeit, Kraft, Schmerz, Quick Dash (Disabilities of the Arm, Shoulder and Hand) und PRWE (Patient Rated Wrist Evaluation) empfohlen. Eine Studie mit einem 10-Jahres Follow-up zeigt signifikante Verbesserungen in den oben erwähnten Outcomes (1).
Die Patientin in diesem Fallbeispiel zeigte initial gute Verbesserungen in allen Messungen, ausgenommen der Beweglichkeit. Das Erlangen einer schmerzfreien Funktion im Alltag stand im Vordergrund der handtherapeutischen Behandlung. Fünf Monate postoperativ nahm die Patientin die Arbeit wieder auf. Ab diesem Zeitpunkt verschlechterte sich der Zustand sowohl subjektiv als auch objektiv.
Die Situation vor und nach der operativen Versorgung mit einer Motec-Prothese ist meist komplex. Erfahrungen zeigen, dass der Rehabilitationsprozess eng begleitet und die Belastungsgrenze gut überwacht werden sollte.
Literatur
- Reigstad, O., Holm-Glad, T., Bolstad, B., Grimsgaard, C., Thorkildsen, R., Rokkum, M., (2017). Five- to 10-Year Prospective Follow-Up of Wrist Arthroplasty in 56 Nonrheumatoid Patients
- Clough, O.T., Lee, G., Hayter, E., Hardman, J., Anakwe, R.E., (2020). Surgery with the Motec total wrist replacement: learning from earlier designs
Conservative treatment of simple proximal phalanx fractures: Dynamic versus Static
M. G. Fioretti1, F. Ferrario1, S. Pagella1, T. Giesen1 (1Gravesano)
Show text
Introduction
Simple fractures to the base and the shaft of the proximal phalanx in fingers in adults, can be successfully treated conservatively. However, static immobilization in safe position has been associated with decreased function after 4 weeks. From 1936, protected immediate mobilization of these fractures has been sought and different splints and protocols have been described that use the Zancolli complex as a main stabilizator of the fractures while promoting early mobilization. We present the results of our review of the literature in this regard.
Method
Articles were sourced from Embase, Medline and Pubmed using the following research words: “phalanx fracture”, “proximal phalanx”, “fracture treatment”, “splint” and “rehabilitation” in various combinations. Inclusion criteria were: conservative treatment of proximal phalanx midshaft and basal fractures.
We looked for:
1) different treatment strategies
2) consolidation rate
3) functional results
4) patients satisfaction
Results
We found 24 articles that could be included in our review.
We found from 1987 a trend towards early protected mobilization of the fractured finger and exclusion of the wrist from the splint.
1)There was no difference in non union and malunion rate between static and dynamic protocols. Dynamic protocols showed best satisfaction of the patients with a lower VAS. Active and passive mobility of the fractured finger was better in patients treated with the dynamic protocol.
2)In case of dynamic regimes with or without wrist immobilization (Hintringer vs LuCa) there was no difference in non union rate or malunion. The LuCa regime, had higher acceptance among patients. Functional recovery was similar in the two groups.
3)Finger only immobilization protocols (buddy strapping) did not show a higher incidence of non-union but a relatively high incidence of radiological malunion (11%), with no clinical correlation. Functional recovery was faster than in other protocols.
Conclusion
Isolated simple fractures of the base and shaft of the fingers phalanxes, seems to have a faster functional recovery with dynamic protocols. Wrist immobilization seems to be unnecessary. Finger only splinting protocols produce a faster recovery with a higher rate of malunion.
References:
1 Strickland JW et al, 1982
2 Jahss SA, 1936
3 Reyes F and Latta L, 1987
4 Pezzei C., M. Leixnering, W. Hintringer, 1993
5 Franz, 2010
6 Woon Man Fok M. et al, 2013
7 Verver et al, 2017
8 Franz ,2012
-
09:30 – 10:00
Kaffeepause
-
10:00 – 11:30
Gartensaal 1 A-C
Hauptsession III
Passion Kinderhand
D. Weber, Zürich (CH) / C. Dufour, Lausanne (CH)Greifen und Begreifen: Die Entwicklung der Kinderhand
M. von Rhein, Zürich (CH)
Unbegreiflich!
D. Weber, Zürich (CH)
Kamptodaktylie: Aetiologie und chirurgische Therapieoptionen
T. Christen, Lausanne (CH)
Kamptodaktylie: Konservative Therapie
C. Dufour, Lausanne (CH)
Kamptodaktylie: Therapieoption mit Glove Splint
M. Schelly, Hamburg (DE)
Sehnenverletzungen der Kinderhand: Chirurgie der Sehnenverletzungen bei Kindern
S. Christen, St. Gallen (CH)
Sehnenverletzungen der Kinderhand: Rehabilitation von Sehnenverletzungen bei Kindern: A family affair
E. Würth, Zürich (CH)
Alles nur lustig? Die Spital-Clown*Innen
als Teil des Therapieteams
J. Winistörfer, Zürich (CH)
-
10:00 – 11:30
Gartensaal 2
Freie Mitteilungen II
C. Bollmann, Lausanne (CH) / T. Giesen, Luzern (CH)Semi-occlusive dressing therapy versus surgical treatment in fingertip amputation injuries
T. Pastor1, P. Hermann1, L. Haug1, B. Gueorguiev2, T. Pastor2, E. Vögelin1 (1Bern; 2Davos)
Show text
Introduction: Treatment of fingertip amputations is still subject of controversial debate. Within the past few years semi-occlusive dressings have increased in popularity for treating this kind of injuries. The aim was to compare conservative semi-occlusive dressing therapy with surgical treatment, with regards to functional outcome, complication rates and patient satisfaction.
Methods: 84 consecutive patients with amputated fingertips and a mean age of 45 (range 19-80) years were re-examined after a mean f-up of 28 (range, 10-46) months. 66 patients (79%) were treated with a semi-occlusive dressing (group 1) and 18 (21%) underwent surgery (group 2) of which 6 (33%) received stump treatment with primary wound closure, 4 (22%) a replantation of the fingertip, 3 (17%) a composite graft, 3 a cutaneous flap and 2 (11%) a neurovascular flap. At final follow up loss of DIP movements, loss of strength and loss of 2-point-discrimination as compared to the uninjured side were measured. Furthermore, VAS, Quick-DASH, aesthetic outcome and loss of working days were obtained.
Results: Group 1 achieved healing in all 66 patients (100%) while group 2 failed in 5 of 18 patients (28%) after a mean of 17 (range 2-38) days. Reason for failure was graft necrosis in all patients. In group 1 mean loss of DIP flexion (3.8° ± 5°) and mean loss of grip strengths (2.9 Kg±6) were lower compared to group 2 ((10.6° ± 19) and (3.9Kg ± 9))(p=0.45 and p=0.99). Mean loss of DIP extension (0° ± 0) and mean loss of 2-point discrimination in group 1 (1mm ± 1) were similar compared to group 2 (0° ± 0) and (0.9mm ± 2)) (p=1 & p=0.88). Mean loss of Pinch strengths was significantly lower in group 1 (0.8Kg ± 1) vs. group 2 (0.5Kg ± 1) p=0.03. In group 1 mean VAS scores (0.2±1) and mean Quick-DASH scores (0.9% ± 2) were significantly lower vs. group 2 ((1.4 ± 2) and (4% ± 12%)) (p<0.001 and p=0.05). Aesthetics was significantly higher in group 1 (86.7% ± 17) vs. group 2 (77.2% ± 17)(p=0.001). Absence from work was significantly shorter in group 1 (28.2 days± 23) vs. group2 (61.7 days ± 30)(p<0.001).
Conclusions: Semi-occlusive dressing for fingertip amputations showed a healing rate of 100%. Compared to surgical therapy similar clinical outcomes, lower complication rates and significantly higher satisfaction rates were achieved with significantly shorter work absence. Hence, semi-occlusive dressing for fingertip injuries is a very successful procedure and should be preferred over surgical treatment.
"One fits all" – Gilt das auch für den SCIP-Lappen in der Handchirurgie ?
E. Fritsche1, T. Giesen1, U. Hug1 (1Luzern)
Show text
Einführung
Der SCIP-Lappen ist wohl im Bereich der rekonstruktiven Chirurgie der Lappen, der dank Super-Mikrochirurgie-Techniken in den letzten Jahren den grössten Hype erlebt hat. Er wird in der Head-and Neck-Chirurgie, der Chirurgie der unteren Extremitäten, der Sarkomchirurgie, ja selbst bei Brustrekonstruktionen immer häufiger eingesetzt. Ist der Lappen auch in der Handchirurgie universell einsetzbar und brauchen wir in Zukunft nur noch diesen einen Lappen. Eine Analyse im eigenen Patientengut soll Aufschluss ergeben.
Methode und Material
Wir haben 10 Patienten mit unterschiedlichen Weichteildefekten an der Hand untersucht. Die Defekte variieren stark in der Grösse der Defekte von 2x4 cm bis 20x8 cm. Es finden sich sowohl palmare wie dorsale Defekte, die Patienten sind unterschiedlich alt von Kindern bis älteren Patienten. Einige Lappen wurden als Notfall-Lappen durchgeführt, die Mehrheit aber als geplanter Eingriff. Ihnen gemeinsam ist aber, dass alle Defekte mit freien mikrovaskulären SCIP-Lappen gedeckt wurden. Dürfen wir daraus folgern, dass dies der Lappen ist, der für schlicht alle Weichteildefekte an der Hand 1. Wahl sein soll im Sinne von "one fits all" ?
Resultate
Alle 10 Lappen an der Hand wurden erfolgreich durchgeführt. In einem Fall zeigte sich eine partielle Nekrose der Lappenspitze. Nur in einem Fall wurde eine sekundäre Lappenausdünnung mit der Patientin diskutiert. Die Lappen können sehr dünn gehoben werden, können bei Bedarf Perforator-chimär gehoben werden und haben den besten Hebedefekt, den man erhalten kann.
Zusammenfassung
Der SCIP-Lappen wird zurecht auch in der Handchirurgie so gehypt und als Lappen der 1. Wahl für praktisch alle Weichteildefekt an der Hand angesehen. Lediglich ganz kleine Lappen an den Fingerkuppen sind Areale, in denen der SCIP-Lappen nicht eingesetzt werden soll, im übrigen aber erfüllt er die Kriterien für "one fits all". Allerdings sind Super-Mikrochirurgie Techniken für die Anwendung unabdingbar. Als Konsequenz ist vorzuschlagen, dass der SCIP-Lappen an den Kliniken für Handchirurgie bevorzugt gelehrt wird.
Mid-term Clinical Outcome of Microvascular Gracilis Muscle Flaps for Defects of the Hand
T. Pastor1, L. Haug1, D. Merky1, R. Meier1, R. Olariu1, E. Vögelin1 (1Bern)
Show text
Introduction: Patients with large soft tissue defects after trauma or infection remain surgically challenging. Gracilis muscle flaps are useful to cover defects of the palm or the distal forearm and hand because they are less bulky than fasciocutaneous flaps. The aim of this study was to analyse mid-term results of gracilis muscle flap coverage for defects on the hand, with regards to functional and aesthetic integrity within the hand.
Methods: 16 consecutive patients with a mean age of 44.3 (range, 20 to 70) years at time of the gracilis muscle flap were re-examined clinically after a mean follow-up of 22.8 (range, 3-77) months. The mean defect size was 124 cm2 (range 52– 300 cm2) which was located palmar (n=9, 56%), dorsal (n=6, 38%) or radial (n=1, 6%). 10 patients had defects after major trauma including bone, joint, tendon and nerve injuries. 6 patients had defects after infections, mainly caused by beta haemolytic streptococci. All flaps were performed as microvascular muscle flaps, covered by split thickness skin graft. Absolute wrist movement, grip strength and reported subjective outcome (1=excellent; 4=poor) were obtained.
Results: Gracilis muscle flaps survived in all patients (100%). However, 6 patients (38%) required reoperations. Reasons for revisions were failure of the venous anastomosis (n=1, 6%) with successful venous revascularisation; one necrosis at the tip of the flap (n=1, 6%) with renewed split thickness skin cover. In two patients a surplus of the flap (n=2, 13%) required flap thinning and in 2 patients with scar contractions (n=2, 13%) scar corrections were performed. Mean wrist flexion/extension was 52° (range, 20-80°) and 42° (range, 0-70°) at final follow-up. Mean grip strength was 23 kg (range 17-29 kg) and mean patient reported satisfaction 1.3 (range 1-2).
Conclusions: Coverage of large defects on the hands with a gracilis muscle flap showed a survival rate of 100%. Patients showed good clinical outcomes with acceptable wrist movements and grip strengths as well as high reported satisfaction rates. Compared to the use of fasciocutaneous free flaps, the pliability and thinness especially on the palmar aspect of the hand is satisfactory. Hence, covering of large defects of the hand with a gracilis muscle flap can be a very successful procedure.
Microsurgery training without living animals : a new approach
C. Bouvet1, N. Balagué1, E. Gjika2, J. Y. Beaulieu2 (1Sierre; 2Genève)
Show text
Teaching microsurgery skills remains challenging without having access to a living animal model. Our idea was to develop a training program that does not require using a living model, which would therefore call for less infrastructure and resources.
The training program is divided into different sections:
- An e-learning section allowing students to access the theoretical knowledge pertaining to the main topics of microsurgery, namely the basics of microsurgery and nerve and vascular suturing.
- A practical section that does not include an animal model which would be a low cost model to allow students to warm up to the different microsurgical skills. This part is divided into different sections that allow a progressive practical approach in 3 steps. First, we focus on DEXTERITY with the “round the clock” and the grape dissection models. Secondly, we focus on a SIMPLE surgical suture on a latex matrix placed around the clock. Lastly, we focus on surgical knots done UNDER PRESSURE, for example in angles, and on dissecting a grape placed in an angle.
- The last step before reaching the animal model is vascular suturing on a tube.
- The practical skills section on the animal model is done on a chicken thigh, where a catheterized system containing food colorant will allow the students to practice suturing the pedicle. Multiple sutures can be performed on this model, namely nerve sutures, autografting, and arterial and venous sutures (in an end-to-end, end-to side and bypass fashion). The irrigation system in place allows to test the patency of the different sutures.
The training program is made up of 9 teaching sessions of 4 hours each (amounting to 36 hours of practice) followed by an exam with a theoretical part (multiple choice questions) and a practical skills part (setting up the catheterized system, nerve and vascular suturing).
We believe that this low-cost teaching approach is a valid alternative to the living animal model currently used to teach microsurgery skills.
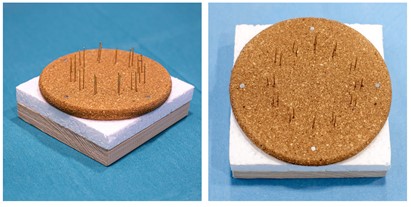
Round the clock training 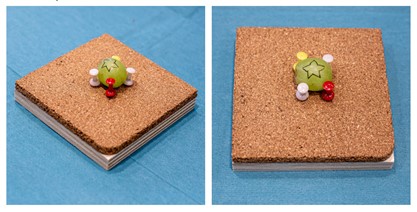
Grape dissection. 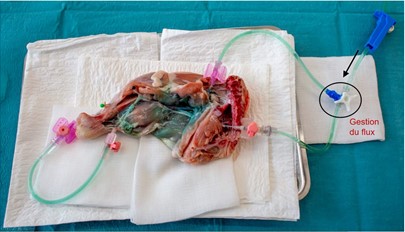
Chicken thigh dissection with veinous and arterial catheterism allowing food colorant to simulate circulation Surgical repair of arthroscopically-induced lesions of the axillary nerve in the blind zone.
C. Dumont1, A. Schneeberger1 (1Zürich)
Show text
Background:
The axillary nerve is at risk during shoulder surgery. Recently, a new type of arthroscopic axillary nerve lesions has been described in the so-called blind zone, the area behind the inferior glenohumeral joint capsule. The surgical treatment of these lesions is challenging because the nerve cannot be directly visualized, and a nerve repair or reconstruction requires generally a combination of surgical approaches.
Three different approaches can be used to repair the axillary nerve: the delto-pectoral-, the axillary- and the posterior approaches. Extended approaches consisting in releasing muscle, like the conjoint tendon, the latissimus dorsi tendon and the long head of the triceps have been further described to increase the visualization of the axillary nerve, respectively.
Goal:
Based on the treatment of 3 patients and a cadaver study on 2 shoulders, we propose a surgical algorithm for the surgical repair or reconstruction of the axillary nerve in the blind zone.
Method:
Three patients with a significant arthroscopic damage of the axillary nerve in the blind zone have been operated on. In 2 cases, the nerve was partially transected and in one case the nerve was sutured to an anchor. Twice, a direct nerve coaptation was performed, and in one case a reconstruction with allograft-interposition was done. In a cadaver study, the amount of axillary nerve exposure and the feasibility of direct nerve repairs or graft interposition were studied in the blind zone using a combination of delto-pectoral, posterior and axillary approaches.
Result:
Using either a delto-pectoral or a posterior approach alone allows only for partial visualization of the axillary nerve, and is not suitable for a direct nerve coaptation using epineural sutures in the blind zone, because of the missing place for surgical instruments. A combination of an extended delto-pectoral approach with release of the conjoint tendon and a limited posterior approach allowed the treatment of complete and partial axillary nerve damages (with or without nerve defects) using a pull-through technique with an artificial nerve conduit or a nerve allograft. The axillar approach did not allow a retrieve of the distal nerve stump if this one was retracted below the insertion of the teres major and latissimus dorsi bone insertions.
Conclusion:
This study showed the feasibility of axillary nerve repair or reconstruction in the blind zone using a combined anterior and posterior approach.
Predictive validity of clinical variables for outcome after cubital tunnel release surgery
N. de Lambilly1, L. Wigger2, M. Papaloïzos3 (1Meyrin; 2Lausanne; 3Genève)
Show text
Objective: Entrapment of the ulnar nerve at the elbow is the second most common compression neuropathy. When operative treatment is indicated, literature fails to distinguish an advantageous technique. To our opinion, the surgical outcome is correlated to the stage of compression and the preoperative symptoms duration rather than to the surgical procedure. The aim of this study was to test this hypothesis and determine the predictive value of the stage of compression according to the McGowan/Goldberg (McGG) classification, the conduction studies (ENMG) and the duration of symptoms.
Methods: We performed a retrospective files study of all patients operated between 2006 and 2018 by three senior hand surgeons using a variety of techniques for idiopathic ulnar neuropathy at the elbow. Traumatic lesions and incomplete files were excluded (15 patients). General data, the McGG stage (I, IIA, IIB and III) and pre-operative ENMG results, classified in three stages (mild, moderate or severe), were collected and compared with the clinical postoperative outcome (good or bad), as defined by persistence or augmentation of at least one of three parameters: sensibility, strength or pain.
Results: A total of 215 operations were reviewed (five lost to follow-up). The mean FU was 10.3 months (1-96). A poor outcome was found in 112 cases (52%). Using Chi-square and simple logistic regression tests with alpha level p < 0.05, the three variables McGG stages, ENMG and duration of preoperative symptoms showed independent significant association with surgical outcome. Multivariate logistic regression analysis combining duration of preoperative symptoms with McGG stages resulted in a good prediction model. Its performance was evaluated on a validation data subset using a ROC analysis (area under the curve=0.76, p=0.0005), which was superior to the performance of univariate models.
Conclusions: Our study supports the hypothesis that poor outcomes are mainly related to the severity of the neuropathy according to the clinical stage. Patients with McGG stage III had worse outcomes, independently of the performed surgical procedure. These patients should be informed before surgery about potentially poor results. The association of ENMG stages and duration of preoperative symptoms with the outcome was statistically significant as well, but weaker. Combining the duration of preoperative symptoms with the McGG stage clearly improved the prediction.
Ultra-minimally Invasive Ultrasound-Guided Thread Carpal Tunnel Release: A review of 26 cases
K. Mende1, V. Schmid1, D. J. Schaefer1, A. Gohritz1 (1Basel)
Show text
Background: Ultra-minimally invasive procedures guided by ultrasound have emerged from the overall tendency towards “scarless” surgery and the availability of high-frequency linear probes with improved quality displays. Previous studies have reported that thread carpal tunnel release (TCTR) is an innovative technique to treat carpal tunnel syndrome (CTS), mainly by the inventors themselves. However, there is a lack of independent evaluation of this technique, therefore the objective of this study is to assess TCTR regarding safety, effectiveness, and postoperative recovery time.
Methods: This retrospective study included 26 patients suffering from carpal tunnel syndrome who underwent TCTR. Patients were assessed preoperatively and postoperatively at day 1, week 1, week 3 and week 6 for objective clinical and subjective outcomes including patient related outcome measures (PROMs) such as Visual analogue scale (VAS), Boston Carpal Tunnel Syndrome Questionnaire (BCTQ) and Disability of the Shoulder and Hand Questionnaire (DASH).
Results: Overall, the study included 13 men and 13 women (aged 23 to 89 years), 10 of which were working. Mean surgery time was 28.6 ± 7.5 minutes, 4 patients had both hands operated using TCTR surgery. The average postoperative return time to normal activities of daily living (ADL) was 3.3 ± 2.5 days, pain medication was concluded after 2.4 ± 1.8 days and time to return to work was 5.1 ± 3 days. BCTQ and DASH scores were comparable to the results reported in previous studies showing early decrease of symptoms. Two patients with persistent carpal tunnel symptoms and one case of recurrencent pain after a 6-month symptom free interval required secondary mini open carpal tunnel release (MOCTR) with complete recovery. All three were patients who were treated in the early phase after the first author (KM) started using the TCTR method. No other complications were reported, especially no infection, hematoma, nerve or tendon lesion.
Conclusion: TCTR surgery seems to be a safe and reliable technique with the benefit of almost no open wounds and scars and a potentially faster recovery time than compared to open techniques. TCTR requires both ultrasound and surgical skills and has a considerable learning curve. Modifications to the original method allow to safely and reliably reproduce results from earlier studies.
Beugesehnenverletzungen nachbehandelt mit Manchester Short Splint vs. CAM Protokoll – erste Resultate
T. Hauri1, B. Tobler-Ammann1, E. Vögelin1 (1Bern)
Show text
Einleitung: Der Trend der handtherapeutischen Behandlung geht bei Beugesehnenverletzungen klar in Richtung frühe aktive Mobilisation. Das bewährte Nachbehandlungsschema «Controlled active motion» (CAM) wird in immer mehr Institutionen durch das «Manchester Short Splint» (MSS) Schema ersetzt. Bei letzterem reicht die Schiene nur knapp über das Handgelenk und der Patient darf von Beginn die Hand für leichte Alltagstätigkeiten einsetzen.
Ziel: Das Ziel dieser retrospektiven Datenanalyse ist es, die Ergebnisse der ersten MSS Patienten aus den Jahren 2020/21 zu präsentieren und mit einer gleich grossen Gruppe von CAM Patienten zu vergleichen.
Methoden: Alle MMS Patienten mit einer primären Beugesehnennaht in den Zonen I oder II im 2020 bis Juli 2021 wurden eingeschlossen. Die CAM Kontrollgruppe wurde nach den Eigenschaften Alter, Geschlecht, verletzter Finger, Zone der Verletzung und Beruf passend aus einem bestehenden Patientenpool zusammengestellt. Die erhobenen Daten wurden deskriptiv analysiert.
Ergebnisse: Bis im Mai 2021 konnten wir 5 MMS Patienten dokumentieren. Diese MMS Patienten hatten ein Durchschnittsalter von 34.2±11.9 Jahren verglichen zur CAM Gruppe mit 30.2±6.4. In beiden Gruppen waren nur männliche Patienten mit jeweils 3 handwerklichen Berufen. In beiden Gruppen waren 1x der Zeigfinger, 1x der Ringfinger und 3x der kleine Finger verletzt. Davon waren 4 Finger in der Zone II und ein Finger in Zone I verletzt.
Die MSS Gruppe zeigte eine Total Active Motion (TAM) von 185±30.4° nach 6 Wochen und 213±18.8° nach 13 Wochen, verglichen mit der CAM Gruppe mit 191±33.8 und 231.2±41.5°. Das Streckdefizit in den PIP Gelenken war mit -11° in beiden Gruppen vergleichbar. In der Woche 13 erreichte die MMS Gruppe im DASH durchschnittlich 13.4±12 und die CAM Gruppe 7.71±3 Punkte. Die Zufriedenheit mit der Hand wurde mit durchschnittlich 7.8±1.5 Punkten in der MSS und 8.4±8 in der CAM Gruppe nach 13 Wochen gewertet. Die Handkraft betrug nach 13 Wochen bei den MSS Patienten durchschnittlich 40±4 kg und bei den CAM Patienten 29.6±4.1. Die MSS Patienten benötigten durchschnittlich 12.3±3.3 und die CAM Patienten 15.8±6.4 Therapiesitzungen bis zum Therapieabschluss.
Schlussfolgerung: Das MMS Schema kann in der Praxis angewendet werden. Die Ergebnisse des neuen Nachbehandlungsschemas MSS sind bei den ersten Patienten mit den Resultaten des CAM Protokolls vergleichbar. Für Patienten mit guter Compliance scheint das MMS Schema ein Vorteil.
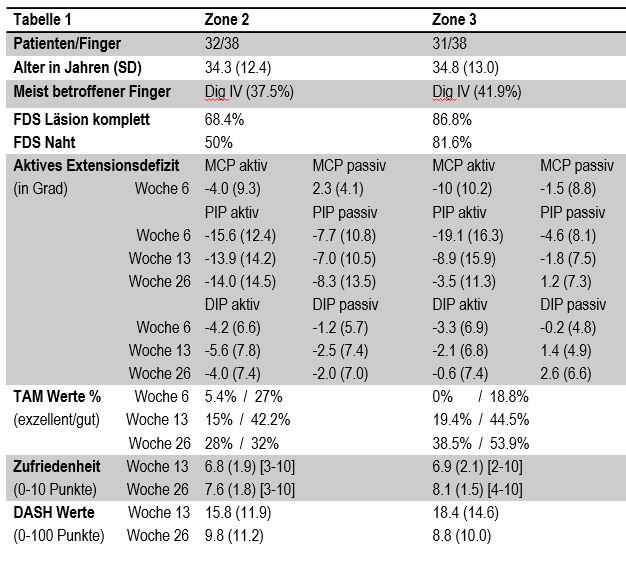
Bewegungsumfang nach Beugesehnenverletzungen Zonen II und III: Retrospektive Fall-Kontroll-Studie
B. Tobler-Ammann1, V. Beckmann-Fries2, M. Calcagni2, A. Kämpfen3, L. Schrepfer3, E. Vögelin1 (1Bern; 2Zürich; 3Basel)
Show text
Einleitung: Zone 3 Beugesehnenläsionen sind mit 13% in unserer multizentrischen Studie weniger häufig als jene der Zone 2 mit 72%. Beschriebene Komplikationen in der Zone 3 sind limitierte Fingerextension und -flexion aufgrund von Verklebungen zwischen Beugesehnen und Lumbricales, sowie der in Flexion gelagerten MCPs. Das Ziel dieser Studie war es, retrospektiv den Bewegungsumfang (ROM: range of motion und TAM: total active motion) in der Zone 3 mit einer Zone 2 Kontrollgruppe nach 6, 13 und 26 Wochen zu vergleichen.
Methode: Einschlusskriterium war eine primäre Beugesehnennaht in der Zone 2/3 mit einer FDP Beteiligung von ≥50% aller Langfinger. Reine FDS Verletzungen wurden ausgeschlossen. Die Zone 2 Gruppe wurde primär nach dem Verletzungsausmass der FDS Sehne (intakt – teilverletzt – durchtrennt) auf die Zone 3 Gruppe abgestimmt, da dieses ein signifikanter Prädiktor für ROM in der Zone 2 und 3 ist.
Resultate: Eine Übersicht ist in Tabelle 1 aufgelistet. Alle Finger wurden mit einer 4-6 Strand-Naht versorgt und frühfunktionell in einer dorsalen Schiene nachbehandelt. In beiden Gruppen wies das MCP nur in der Woche 6 ein aktives Extensionsdefizit auf. Das PIP und DIP wiesen in beiden Gruppen zu allen Messzeitpunkten ein aktives Extensionsdefizit auf. Die TAM Werte wurden in beiden Zonen über die Zeit ähnlich besser, wobei es in der Zone 3 nach 26 Wochen deutlich mehr exzellente und gute Bewertungen nach Tang gab (92.4%) als in Zone 2 (60%). Die Handkraft betrug in der Woche 13 51% (Zone 3) und 59% (Zone2), nach 26 Wochen 84% (Zone 3) und 79% (Zone 2). Die subjektive Zufriedenheit und der DASH waren in beiden Gruppen ähnlich.
Schlussfolgerung: Die beschriebenen Komplikationen in der Zone 3 spiegeln sich nicht in unseren Resultaten. Die Extensionsdefizite in der Zone 3 sind generell kleiner als in der Zone 2. Ebenso erholt sich die aktive wie passive ROM in der Zone 3 besser und schneller als in der Zone 2, was die Unterschiede in den TAM Werten ausmacht. Punkto Therapie, Kraft, DASH und Zufriedenheit sind die Gruppen jedoch ähnlich. In der Praxis muss in beiden Zonen dem PIP besonders Beachtung geschenkt werden, um Extensionsdefizite möglichst zu minimieren.
Resultate_Zone_2_3.JPG Extensor digiti minimi to Abductor pollicis brevis tendon transfer for palmar abduction of the thumb
N. Riteco1, S. Schibli1, J. Fridén1 (1Nottwil)
Show text
Purpose:
Loss of palmar abduction of the thumb e.g. after a median nerve lesion, impairs positioning of the thumb for grasping as well as the control and direction of force in key-pinch. We describe a method for the restoration of palmar abduction of the thumb using the extensor digiti minimi (EDM) to abductor pollicis brevis (APB) tendon transfer and present clinical outcomes.
Methods:
The tendon of the EDM is severed at the MCP-V joint, mobilized proximally and subsequently passed through the interosseous membrane from dorsal to palmar, proximally to the pronator quadratus muscle. The tendon is then guided from deep to superficial ulnar to the FCR tendon, which serves as a pulley. Finally, the tendon is routed subcutaneously and attached to the insertion of APB.
From 2010 to 2019 we performed 11 EDM to APB tendon transfers in 10 patients as a part of grip reconstruction. 9 patients were tetraplegic, one patient was paraplegic with an additional lesion of the lower brachial plexus.
Results were measured for 6 patients 6 and 12 months after surgery using the grasp and release test (GRT) in which the patient has to perform a series of tasks within a certain time limit.
Results:
All patients achieved an active palmar abduction of the thumb.
In the 6 patients for whom data was available we saw a median increase in GRT from 69.8 points preoperatively to 160.8 points 12 months after surgery.
Conclusion:
Palmar abduction of the thumb is crucial for hand opening in order to grasp. We describe a method to achieve active palmar abduction with a transfer of the EDM to APB tendon with good results. The line of action of the donor tendon is straight. With immediate postoperative active mobilization, adhesion formation can be avoided. We see indications for this reconstruction in patients with a low tetraplegia, lower plexus injury and median nerve palsy.
Since the goal of this tendon transfer is a better positioning of the thumb for grasping and not to increase the force of the key-pinch, we also consider this transfer when the donor EDM muscle has a force of less than M4. This opens the field for a possible tendon transfer of a previously reinnervated EDM muscle after nerve transfer in higher tetraplegia.
Covering of Mini-Plates with Flexor Pulleys in the Treatment of Dorsal Fracture-Luxation of the PIJ
M. Maniglio1, E. Zaidenberg2, J. Sanchez Saba2, J. Boretto2, G. Gallucci2, P. de Carli2 (1Lausanne; 2Buenos Aires AR)
Show text
Introduction
In the treatment of Dorsal Fracture-Dislocations (DFD) of the Proximal Interphalangeal Joint (PIP) a palmar surgical approach has the advantage of an optimal visualization of the articular surface and the placement of the mini-plate in a buttress position to hold the fragments in reduction, especially important in fractures where small articular fragments aren’t suitable for a screw fixation. However, the extensive dissection of the volar tissues could lead to increased post-operative stiffness and adhesions with flexor contractions, reduction of range of motion (ROM) and secondary plate removal. We want to introduce a technic of an additionally coverture of the mini plate with the flexor tendon pulleys, who may further reduce the adhesion between the mini-plates and the tendons and so reduce postoperative complications.
Methods
This retrospective consecutive case series includes 4 male patients with an average age of 32 years (range 26-55 years). Mean time between trauma and surgery was 11 days. We treated our patients with a locking titanium mini-plate and 1.5-mm-diameter screws for DFD of the PIP, the mean involved part of the articulation was 37% (range 30-45%) and one patient out of four had an articular comminution. The mean follow-up was 8 months (range 6-13 months).
Results
All fractures healed clinically and radiographically by 6 weeks. All patients were satisfied with the clinical results and returned to their prior work. Mean active ROM values at final follow-up were: PIP flexion 96°, PIP extension 7,5°, DIP flexion 65°, and DIP extension 11°. The mean pain Visual Analog Score was 0.25 and the Quick-DASH Score 1.75.
Discussion
With the help of a flap out of the flexor tendon sheath and the pulley system, the hardware is covered after ORIF of the fracture producing a gliding layer between the hardware and the deep flexor tendon. The theoretical drawback of a bowstringing of the flexor tendon exists, but the venting of the A4 pulley was showed of no clinical consequences in prior studies. So that the beneficial effect of this technique outruns the negative effects of the partial sacrifice of the A4 pulley. In our presented case series, we had excellent results in all four patients without complications.
Conclusion
In conclusion this study presents a surgical technic who may potentially reduce the high complication rate found after ORIF for DFD-treatment of the PIP, restoring patient’s satisfaction with good clinical outcomes.
-
10:00 – 11:15
Vortragssaal 2
Workshop 2
B. Roland, Miège (CH)Stack’sche Schiene aus Orfitcast: alltagstauglich und atmungsaktiv
L. Scheurer, Bern (CH)
Mit freundlicher Unterstützung: Hermap AG, Ebikon
Show full description
Im Workshop lernst du eine Stack’sche Schiene aus dem atmungsaktiven Schienenmaterial Orfitcast herzustellen. Durch die hohe Atmungsaktivität des Materials kann die Schiene bei den meisten Klienten 8 Wochen non-stopp getragen werden und gewährt so eine optimale Lagerung des Mallet-Fingers. Die Schiene wird simpel mit Tape am Finger befestigt und gewährt somit einen super sicheren Halt im Alltag sowie eine gute Flexion des MP und PIP ist möglich.
-
11:30 – 13:00
Stehlunch – Begegnung in der Ausstellung
-
11:45 – 12:30
Gartensaal 1 A-C
Mittags-Symposium 3
Advanced Patient Specific Tools for Corrective Osteotomies of the Wrist and Forearm
PD Dr. med. Philipp Honigmann, Liestal / Dr. med. Mathias Häfeli, Chur
-
11:45 – 12:30
Gartensaal 2
Mittags-Symposium 4
TOUCHable? KERIFLEXible? MOTEChnical?
Elvira Bodmer, Luzern / Urs Hug, Luzern
-
11:45 – 12:30
Vortragssaal 2
Session Junge Handchirurgen
Schweiz
-
13:00 – 14:30
Gartensaal 1 A-C
Hauptsession IV
Mains de musicien
C. Bouissou, Annemasse (FR) / P. Cuénod, Genève (CH)Pathologies chirurgicales de la main du musicien
F. Mauler, Aarau (CH)
La dystonie de fonction ou la mort symbolique de l’artiste
A. Hauser-Mottier, Genève (CH)
Traitement des fractures de la main et du carpe chez le musicien
P. Cuénod, Genève (CH)
Vision globale du musicien et concepts de prise en charge ergothérapeutique
C. Bouissou, Annemasse (FR)
Michel Tirabosco, la musique malgré un handicap
P. Cuénod, Genève (CH)
-
13:00 – 14:30
Gartensaal 2
Freie Mitteilungen IV
Communications libres IV
C. Wyss, Basel (CH) / P. Grosclaude, Sion (CH)The effectiveness of vacuum therapy for the treatment of scars: a literature review
M. de Ieso1 (1Sierre)
Show text
Introduction: An important part of the activity of hand therapists includes the treatment of scars. Complications such as: hypertrophic tissue, adhesion formation, pain, pruritus or joint contracture can occur and must be prevented (Burke et al., 2006). Among the non-invasive scar treatment techniques, Monstrey et al. (2014) quote the massage. Vacuum therapy performed by a device, is one of the method available for massaging scars.
Objectives: What are the physical and physiological impact of the vacuum therapy on the skin? What are the indications for its use on scars?
Methods: A review of the literature has been conducted (Swiss Consortium, Cochrane Library and Google Scholar) to synthesize the principles of vacuum therapy and to issue practical guidelines. These findings were confronted with the recommendations issued by the firm that supplies the vacuo-depression device Skin V6®.
Results: Sixteen publications were included for a qualitative synthesis. In terms of physiological impact, depressomassage provokes the accumulation of longitudinal collagen bands in the subcutaneous tissue accompanied by an alteration of fibroblasts (Adock et al., 1998, Adock et al. 2001 and Meirte 2016). The main physical benefits highlighted are the reduction of the hardness of the skin and the improvement of elasticity.
Conclusion: An empirical approach which takes into account the stage of healing and the characteristics of the impairment must guide the use of this technique. In terms of device settings, the data shows that the type of massage performed by the head has more impact than the suction force on the skin.
Adcock & al. (1998). Continuing Medical Education Examination Body Contouring : Cutaneous and Systemic Effects of Endermologie in the Porcine Model. Aesthetic Surgery Journal, 18(6), 414–420.
Adcock & al. (2001). Analysis of the Effects of Deep Mechanical Massage in the Porcine Model. Plastic and Reconstructive Surgery, 108(1), 233–240.
Burke & al. (2006). Hand and Upper Extremity Rehabilitation (3rd ed., p.39-40). Churchill Livingstone.
Meirte & al. (2016). Short-term effects of vacuum massage on epidermal and dermal thickness and density in burn scars: an experimental study. Burns & Trauma, 4, 1–9.
Monstrey & al. (2014). Updated Scar Management Practical Guidelines : Non-invasive and invasive measures. Journal of Plastic, Reconstructive & Aesthetic Surgery, 67(8), 1017–1025.
Paraffinrecycling- ein Nachhaltigkeitsprojekt
E. M. Gleiser1, B. Brown2 (1Thalwil; 2Zürich)
Show text
In der Handtherapie setzen wir regelmässig das Paraffinbad ein, um die Hände für die Therapie aufzuwärmen bzw. um die Durchblutung und Entspannung zu fördern. Das hilft auch oft schon gegen Schmerzen.
Paraffin wird aus Erdöl gewonnen. Auch in der Therapie sollten wir vernünftig und sparsam mit den natürlichen Ressourcen umgehen. Allein schon in unserer Handtherapiepraxis verbrauchen wir 4.5 kg Paraffin pro Woche. Da das Paraffin nach einmaligem Gebrauch entsorgt wird, bedeutet dies ein Abfallvolumen von 234 kg im Jahr. Das ist alles andere als umweltschonend.
In der Imkerei kommt Bienenwachs zum Einsatz, das regelmässig wiederverwendet wird. Gemeinsam mit einem Imker konnten wir ein Paraffin-Recyclingprogramm aufbauen, bei dem das gebrauchte Paraffin gesammelt, gefiltert, gereinigt und für die Therapie neu aufbereitet wird.
Massanz Gina, 2007, Determination of Paraffin Contamination between Users – Final Project Report. Rtech laboratories, St. Paul, MN, USA.
Pratique du violon et allodynie: dilemme.
E. Agneskis1 (1Luxembourg LU)
Show text
La pratique du musicien peut être comparée à celle d’un sportif de haut niveau.Le temps passé à répéter sur son instrument s’assimile aux nombreuses heures d’entrainement journalières d’un athlète visant la perfection du geste.Leur activité physique est à la fois longue et répétitive:69% des musiciens seront confrontés à des troubles musculo-squelettiques(TMS),19% à des problèmes liés aux nerfs périphériques,5% de dystonie focale(autres:7%)au cours de leur carrière(Lederman,2003,De Sousa Moraes,2012).
S, jeune violoniste concourant au 1er Prix du Conservatoire,a subi un traumatisme engendrant une lésion du système nerveux périphérique (SNP),plus particulièrement de neuro-fibres Aβ,générant des mécanismes de réorganisation du système somesthésique au niveau central,s’exprimant en périphérie par une hypoesthésie paradoxalement douloureuse au toucher:l’allodynie mécanique(AM)(McCabe, 2009).
Une lésion nerveuse périphérique peut induire des changements tant au niveau du SNP(Spicher et al. 2008b)qu’au niveau du système nerveux central.En s’appuyant sur la théorie du portillon (Melzack&Wall,1965)qui établit que la stimulation des fibres Aβ bloque les réponses des neurones médullaires nociceptifs,la contre-stimulation vibrotactile à distance induirait donc une inhibition active des douleurs neuropathiques.
Sachant que les gestes répétitifs entraînent plus de contraintes et de stress sur les nerfs périphériques(INRS, 2011),et que les postures que l’on adopte suite à un traumatisme ne respectent généralement pas la physiologie,elles peuvent donc provoquer d’autres pathologies(TMS, …).Or, la première prescription en présence d’un territoire allodynique, est de ne pas le toucher,autant que se peut(Spicher, 2020).Comment permettre à S d'harmoniser sa pratique de la musique,notamment le violon,avec la présence d’une AM sur D3 de la main gauche,avec les gestes et posture du violon, sans perdre en performance musicale ?Un choix s’impose-t-il entre l’appareillage de ce doigt,la rééducation sensitive de la douleur neuropathique,et la pratique musicale?Les contraintes liées à l’un sont-elles conciliables avec les impératifs de l’autre?
L’activité humaine est au cœur du métier de l’ergothérapeute,orchestrant les tentatives d’appareillage, rythmant les approches rééducatives en accord avec les besoins de S, présentant une atteinte par écrasement du nerf collatéral palmo-ulnaire du nerf médian pour D3 de la main gauche,passionnée de musique souhaitant professer dans le domaine.
Prothetischen Versorgungen der oberen Extremitäten, die beim Sport zum Einsatz kommen!
P. Meier1, C. Thienel1, T. Henn1 (1Bellikon)
Show text
Einführung
Trotz der zunehmenden Möglichkeiten der chirurgischen Behandlung und auch der Rekonstruktionsmöglichkeiten bei komplexen Verletzungen, Fehlbildungen oder bösartigen Erkrankungen der oberen Extremität sind prothetische Versorgungen notwendig, um die Funktion und auch die soziale und berufliche Wiedereingliederung zu verbessern. Wie der medizinische Fortschritt haben sich auch die Möglichkeiten und Optionen in der Prothetik entwickelt. Vor allem die Prothesen müssen und können sich an die steigenden Anforderungen junger Patienten im Berufs- und Freizeitleben und vor allem bei sportlichen Aktivitäten sind für Techniker und Material oft eine Herausforderung. Was ist möglich, auf was muss geachtet werden und wie können wir dies erreichen?
Material und Methode
In unserer Klinik werden jährlich etwa 50 Patienten mit Prothesen für die oberen Extremitäten versorgt. Davon werden 50 % mit funktionellen kosmetischen Prothesen, 10 % mit mechanischen Prothesen, 40 % mit Hybrid- und myoelektrischen Prothesen, 20 % davon mit multiartikulären Händen versorgt. Wenn immer möglich, sollte mit der prothetischen Versorgung auch die Bedürfnisse, der sportlichen Aktivität gedeckt sein. Eine reine Sportprothese wird in der Regel, in der Schweiz von den Kostenträgern nicht übernommen.
Ergebnisse
Wir berichten über die unterschiedlichen Bedürfnisse und Möglichkeiten der prothetischen Versorgung der oberen Extremität, welche auch für die verschiedensten Sportarten eingesetzt werden können. Golf, Mountain Biken, Bump Track, Snowboarden und sogar Klettern ist kein Traum, sondern möglich.
Diskussion und Abschluss
Die prothetische Versorgung nach Amputationen der oberen Extremitäten ermöglicht ein unabhängiges Leben mit Rückkehr ins Berufsleben, ein Minimum an sozialer Stigmatisierung und auch eine Rückkehr zum Sport. Dieses Wissen kann dem Handchirurgen bei schwierigen Gesprächen mit Patienten über Amputationen der oberen Extremität helfen und zeigt eine Perspektive für alle Beteiligten auf.
eSportler in der Handtherapie
M. Abt1, R. Glanzmann1, M. Preisig2 (1Sursee; 2Teufen)
Show text
Facts: In der Schweiz beträgt die wöchentliche Spieldauer von eSport und Gamen im Durchschnitt 11 Stunden. 51.8 % der eSportler spielen zu Hause am eigenen PC oder Laptop (Hüttermann M. 2019).
Zu den grössten Beschwerden bei den eSportlern gehören unter anderem mit 42 % Nacken- und Rückenschmerzen, 36 % Handgelenkschmerzen und 32 % Handschmerzen (DiFrancisco-Donoghue J. et al., 2019).
In der Praxis stellen wir fest, dass Patienten immer wieder an einer Repetitive Strain Injury (RSI) leiden. In der Therapie gehen wir bei den Büroangestellten davon aus, dass diese am Arbeitsplatz entsteht. Auf Nachfrage bei unseren Patienten zeigt sich, dass einige nach dem Büroalltag zu Hause eSport betreiben.
Fragestellung: Wie können wir eSportler in der Handtherapie mit RSI unterstützen, damit der Therapieerfolg langanhaltend ist?
Vorgehen: Dazu wurden Datenbanken sowie Erfahrungsberichte und Fachbücher nach Studien zum Thema RSI und eSport durchsucht. Zudem dienten unsere Patienten als Praxisbeispiele.
Ergebnisse: Die gesichtete Literatur zeigt viele Massnahmen und deren Wirkung auf, jedoch mit geringer bis moderate Evidenz. Die daraus entstandene Behandlungsleitlinie, welche die Therapeuten leitet und unterstützt, beinhaltet diverse Aspekte für die Behandlung wie z.B. Assessments, Heimprogramme, Merkblatt zur Ergonomie am Computer etc. Zudem zeigt sie auf, wie komplex die Situation ist und deshalb eine interdisziplinäre Zusammenarbeit notwendig macht. Die Behandlung beinhaltet sowohl die arbeitsbezogenen sowie auch die lebensbezogenen Risikofaktoren.
Schlussfolgerung: Erst eine ganzheitliche Erfassung der Gesamtsituation und Behandlung von eSportler kann einen längerfristigen Behandlungseffekt bei RSI erzielen. Dies zeigt auch das «Integrated Health Management Model» von DiFrancisco-Donoghue J. et al., 2019. Für die Praxis lässt sich zusammenfassen, dass die entstandene Behandlungsleitlinie für die Klienten eingesetzt werden kann und individuell angepasst werden soll.
Literatur:
- DiFrancisco-Donoghue J., Balentine J., Schmidt G., Zwibel H. (2019). Managing the health of the eSport athlete: an integrated health management model. BMJ Open Sport & Exercise Medicine, 5, 1-6.
- Hüttermann M. (2019). eSports Schweiz 2019. Winterthur: ZHAW School of Management and Law. Institut für Marketing Management.
-
13:00 – 14:30
Vortragssaal 2
Workshop 3
P. Kammermann, Bern (CH) / I. Cianci, Affoltern am Albis (CH)Behandlung von Kamptodaktylie und Fingernarbenkontrakturen bei Säuglingen und Kleinkindern - Anfertigung eines Glove-Splints
M. Schelly, Hamburg (DE) / N. Ewers, Hamburg (DE)
-
14:30 – 15:00
Kaffeepause
-
15:00 – 16:30
Gartensaal 1 A-C
Hauptsession V
Best case ever
D. Herren, Zürich (CH)Einführung
D. Herren, Zürich (CH)
Autoren
M. Calcagni, Zürich (CH) / E. Fritsche, Luzern (CH) / T. Giesen, Luzern (CH) / M. Häfeli, Chur (CH) / S. Schindele, Zürich (CH) / A. Schweizer, Zürich (CH) / E. Vögelin, Bern (CH)
Zusammenfassung, Abstimmung, Preisverleihung
D. Herren, Zürich (CH)
-
16:30 – 16:45
Gartensaal 1 A-C
Awards Ceremony
SGHR-Award
Moderation: Michael Haller, Solothurn/Christa Greminger, Zug/ Atena Bosi, Payerne
Gong Show-Award
Moderation: Stephan Schindele, Zürich
Greatest Future Clinical Application Award
Moderation: Stephan Schindele, Zürich
Poster Award
Moderation: Stephan Schindele, Zürich
-
16:45 – 17:00
Gartensaal 1 A-C
Schlusspunkt
U. Hug, Luzern (CH) / M. Calcagni, Zürich (CH) / P. Kammermann, Bern (CH) / S. Rosca-Furrer, La-Chaux-de-Fonds (CH)